Carotid Artery Stenting
Whilst we make every effort to ensure that the information contained in this patient information sheet is accurate, it is not a substitute for medical advice or treatment. The Circulation Foundation recommends consultation with your doctor or health care professional. The information provided is intended to support patients, not provide personal medical advice. The Circulation Foundation cannot accept liability for any loss or damage resulting from any inaccuracy in this information or third-party information, such as information on websites to which we link.
Why Do I Need the Treatment?
Carotid artery stenting may be recommended as part of a treatment plan to prevent stroke. In some cases, a stroke may occur due to a narrowing in the carotid artery in the neck, which provides blood supply to the brain.
If you have recently had a mini-stroke (TIA) and have also been found to have a narrowing in the carotid artery, your medical team is likely to recommend treatment with medications such as blood thinners (e.g., aspirin +/- clopidogrel) and cholesterol-lowering medications (e.g., statins) which are known to reduce future risk of stroke. They may also discuss treatment options to open the narrowed segment of the carotid artery, which may be done through surgery (carotid endarterectomy) or carotid artery stenting.
There are pros and cons of each approach, but stenting may be recommended over surgery if you have previously had neck surgery or radiotherapy, or if surgery may be considered higher risk for you.
In some cases, a narrowing in the carotid artery is found which has not caused any symptoms of a mini-stroke. In certain cases, carotid artery stenting (or surgery) may be recommended to reduce the long-term risk of stroke.
Preparation for the Treatment
Carotid stenting is usually performed under local anaesthetic, but the team may still require you to be fasting beforehand in case sedation is required. The procedure will take place in either an interventional radiology suite or a hybrid operating theatre with X-ray guidance. The keyhole procedure is usually performed through a needle in the groin (femoral artery).
Before the procedure begins, you will have some monitoring placed to measure your blood pressure, pulse, and oxygen saturations, and you may be given some oxygen to breathe.
The Procedure
After the groin area is cleaned with antiseptic solution, a local anaesthetic injection is given to numb the area, and then a needle is introduced via the femoral artery in the groin using ultrasound scanning as a guide. Then, using X-ray guidance, a wire is advanced through the arteries from the groin to the carotid artery in the neck.
There may be a small temporary filter device used, which catches any tiny fragments of debris from the narrowing and prevents these from traveling to the brain and causing a mini-stroke.
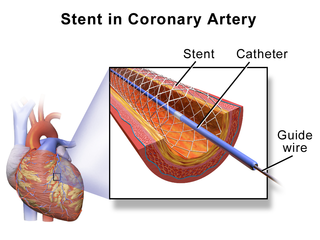
The carotid artery stent is then introduced over the guidewire and placed in the correct position using X-ray guidance and dye. After the stent is placed, it may also be stretched to fully fit the artery by inflating a temporary balloon. This may give some discomfort in the neck for a few seconds and can also make some people feel a little hot or faint. If needed, the team can administer some fluids via a drip to help correct this.
Throughout the procedure, the team will be monitoring you closely and may ask you to perform simple tasks such as squeezing a ball or talking to them. This is to monitor brain function during the procedure.
The whole procedure is likely to take between 1 hour and 1 hour 30 minutes to complete.
After the Treatment
After the procedure, you will need to spend between 2 and 4 hours on bed rest to reduce the risk of bleeding or bruising from the needle site in the groin. The team will continue to monitor your observations and will also check your speech and movements to ensure they are all normal during this time.
After this period of bed rest, the team will check your groin, and if they have no concerns, you will be allowed to sit up and walk around again. You will be able to eat and drink as soon as the procedure is completed.
Going Home
Most people stay in the hospital overnight and go home the following morning. In some cases, you may be allowed home the same day. You can return to normal activities as soon as you feel comfortable. Any bruising in your groin area will usually clear in 5-7 days.
You will be given some blood thinners to take (usually aspirin and clopidogrel) for at least 4 weeks after the procedure and will be asked to continue one of these (usually clopidogrel) lifelong. This is to help prevent the stent from narrowing down or blocking in the future. It is also very important that you do not smoke after this procedure.
You can gradually get back to all your normal activities within a week or so of the procedure, but you should be aware that bruising may happen more easily if you have been asked to take two blood thinners. You are likely to have a scan to check the stent around 4-6 weeks after the procedure and also be reviewed in clinic by the team.
What Can I Do to Help Myself?
If you are a smoker, you should make a determined effort to stop completely. Continued smoking will cause further damage to your arteries and increase the risk of stroke, heart attacks, and problems with the circulation in your legs.
You can also reduce your risk of vascular disease by reducing your weight, eating a low-fat diet, and getting plenty of regular exercise.
If you have high cholesterol or blood pressure, make sure it is checked regularly and that you are on the correct medication.
If you have diabetes, make sure that you monitor your blood sugar levels. Diabetics are more at risk of developing vascular disease due to heightened blood glucose levels, which speed up the furring of the arteries.
Complications
A small number of people, between 1-3 in 100 undergoing carotid stenting, will suffer a stroke during or shortly after the procedure. All possible precautions will be taken to prevent this from happening. If a stroke is suspected, further scans may be required, and the local stroke team will be contacted for advice on any further treatment needed.
Bleeding that causes a clot around the entry wound in the artery in your groin can occur, but it is rarely a problem. In 1-2% of cases, this needs to be removed by a minor operation, but usually, the blood is removed by the body over a period of 1-2 weeks.
If you had to have an angiogram to check the stent placement and blood flow, you may have an allergic reaction to X-ray dye, but this is rare.
If you have other medical conditions such as angina or bronchitis/asthma, these conditions may be aggravated at the time of stenting. This rarely causes a major problem.
Read the leaflet